💡 Use the tool: Model different compensation structures with the free Associate Compensation Calculator.
Why Does Associate Compensation Structure Matter So Much?
Clinician compensation is one of the most negotiated and misunderstood topics in private dental practice. Get the model wrong and you’ll either overpay for low production, underpay and lose a talented hire to a competing offer, or create misaligned incentives that damage the patient experience. In fact, choosing the wrong compensation model is one of five costly financial mistakes that practice owners consistently make — and one of the hardest to reverse once a hire is in place.
For related reading, see our guide on dental staff hiring and compensation.
For related reading, see our guide on efficient dental clinic management.
For related reading, see our guide on growing through patient retention.
For related reading, see our guide on dental practice growth strategies.
According to the American Dental Association’s 2025 Dentist Income and Billing Survey, the median annual income for a full-time associate dentist in private practice was $175,000 — up 8.3% from 2023, driven by strong new dentist demand in suburban and rural markets (ADA, 2025).
For practice owners considering adding an associate as a growth strategy, see our guide on effective growth strategies for dental practices and our detailed analysis of how much dentists make across practice types.
What Is the Percentage of Production Model?
The percentage of production model pays the provider a fixed percentage of the total procedures they complete, regardless of whether those procedures are collected. It’s the most common compensation structure in private practice.
How Production Percentage Is Calculated
Production typically refers to UCR (usual, customary, and reasonable) fees billed — not the insurance-adjusted amount. So if an associate completes a $1,200 crown and the insurance write-off reduces collections to $900, the production basis for the commission is still $1,200.
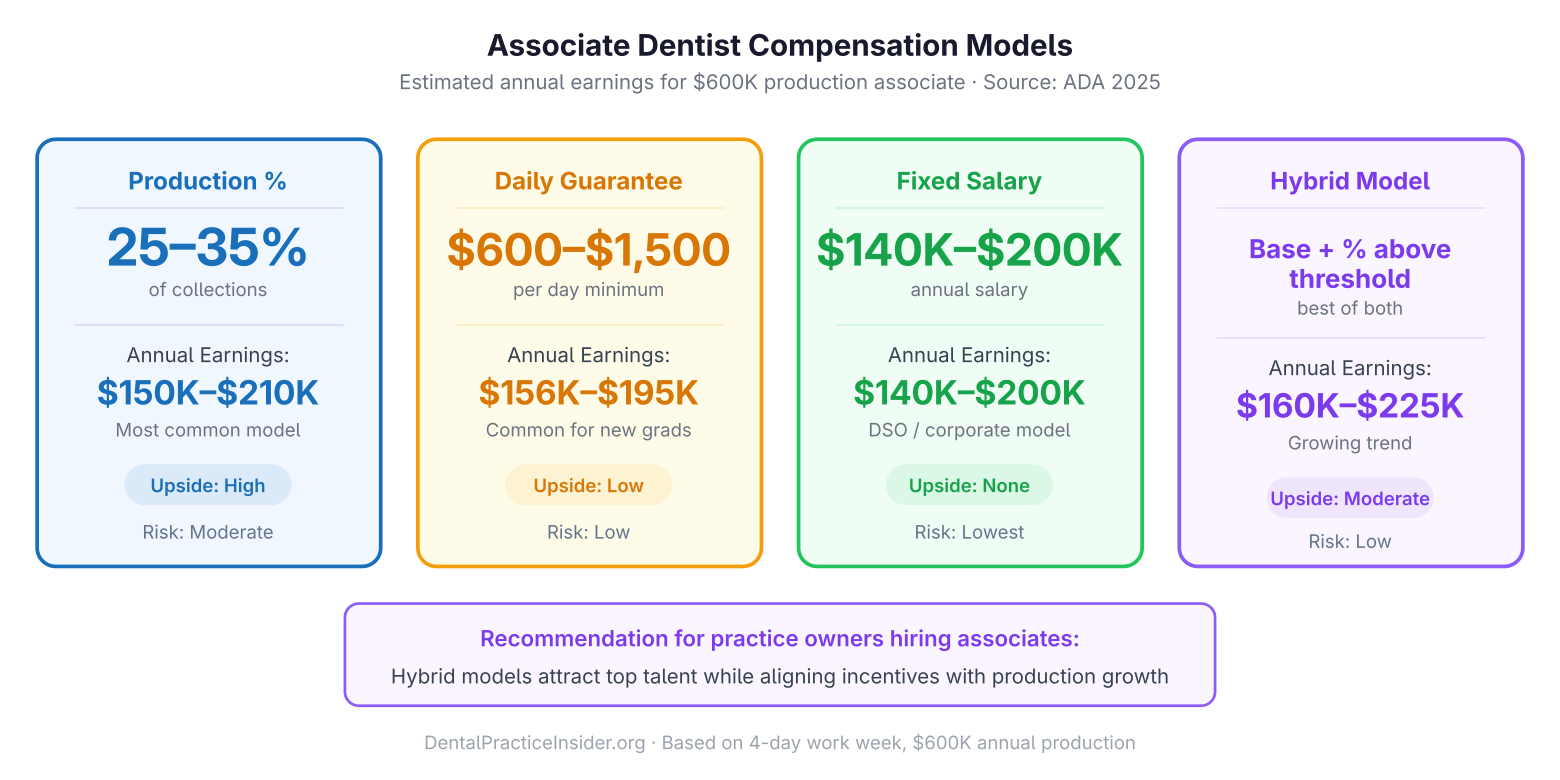
Associate dentists typically earn 25–35% of production, translating to $8,750–$35,000 per month depending on experience level and production volume.
| Associate Type | Typical Production % | Monthly Production Target | Estimated Monthly Income |
|---|---|---|---|
| New graduate (0–2 years) | 25–28% | $35,000–$50,000 | $8,750–$14,000 |
| Experienced (3–7 years) | 28–32% | $50,000–$75,000 | $14,000–$24,000 |
| Senior/specialist level | 30–35% | $70,000–$100,000 | $21,000–$35,000 |
Pros and Cons of Production Percentage
- Pro: Simple to calculate; rewards productivity directly; provider isn’t penalized for insurance claim delays
- Pro: Aligns associate incentives with practice production goals
- Con: Practice owner bears collection risk — if insurance doesn’t pay, the associate’s production commission still accrues
- Con: Can incentivize speed over quality if % is the only metric tracked
What Is the Percentage of Collections Model?
The collections percentage model pays the clinician based on what the practice actually collects for their procedures, not what was billed. This shifts collection risk to the provider.
Typical collections percentages run slightly higher than production percentages — 30–38% — to offset the collection risk. In a well-run practice with a strong billing department and high collection rates (95%+), the difference between production and collections percentage may be minimal. In practices with high write-offs or insurance collection delays, the gap can be significant.
When Collections Percentage Makes Sense
Collections percentage is appropriate when:
- The practice has a high percentage of uninsured patients paying out of pocket (collection rate uncertainty is lower)
- The practice has a membership plan model where collections = production
- The associate has significant control over the billing process
What Is a Daily Guarantee and When Should You Use It?
A daily guarantee (also called a day rate or minimum guarantee) pays the associate a fixed amount per day worked, regardless of production. It’s most commonly used for:
- New hires in their first 90–180 days while they build speed and establish a patient base
- Part-time providers working 1–2 days per week in a practice they don’t fully control
- Associateships in low-volume practices where production consistency is uncertain
Daily Guarantee Rate Benchmarks (2026)
| Experience Level | Daily Guarantee | Annual Equivalent (4 days/week) |
|---|---|---|
| New graduate | $600–$800/day | $125,000–$166,000 |
| 3–5 years experience | $800–$1,100/day | $166,000–$228,000 |
| Specialist (GP with implant/endo skills) | $1,000–$1,500/day | $208,000–$312,000 |
Daily guarantee arrangements are typically temporary or used as a floor with a production upside. A common structure: “daily guarantee of $700, or 30% of production, whichever is greater.” This protects the clinician during slow periods while giving the practice upside when the associate produces above the break-even threshold.
What Is a Hybrid Compensation Model?
Hybrid models combine elements of multiple structures to align incentives at different production levels:
- Tiered production percentage: 27% on production up to $60,000/month, 32% on production above $60,000. Rewards high producers with a higher marginal rate.
- Base salary + production bonus: Fixed annual salary ($130,000–$150,000) plus a quarterly production bonus if production exceeds a threshold. Provides security for the associate while retaining upside for the practice.
- Guarantee + production percentage: As described above — floor protection with uncapped upside.
What Benefits Are Typically Included in Associate Packages?
Beyond base compensation, a competitive associate package in 2026 includes:
- Malpractice insurance (occurrence or claims-made — understand the difference)
- DEA registration reimbursement
- State dental license fee reimbursement
- CE allowance ($1,500–$3,000/year)
- Health insurance contribution (50–75% of premium)
- Paid vacation (10–15 days) and sick days
- 401(k) with employer match (increasingly common in corporate and DSO settings)
Benefits that are non-negotiable deal-breakers for most new doctors: malpractice coverage and CE allowance. Benefits that differentiate offers in a competitive market: health insurance contribution and student loan assistance programs.
What Contract Considerations Should Associates and Owners Watch For?
Non-Compete Clauses
Non-compete agreements in dental contracts typically restrict the associate from practicing within a specified radius (5–10 miles) for 1–3 years after departure. Enforceability varies significantly by state — California, North Dakota, and Minnesota have effectively banned non-competes, while most other states enforce them if they’re “reasonable” in scope. Have an attorney review any non-compete before signing.
Patient Ownership Language
Contracts should clearly state that patients are patients of the practice, not the provider. This protects the practice if the clinician departs and prevents disputes about who can contact departing patients.
Termination Clauses
Look for “at-will termination with 30–90 days notice” language. Shorter notice periods favor the practice; longer periods favor the associate. Both parties benefit from a mutual 60-day notice provision that allows adequate transition planning.
Does a Partnership Track Change the Compensation Equation?
When a practice owner offers a pathway to ownership or partnership, the initial compensation package often looks different — sometimes lower in base rate, with the understanding that equity is being accumulated or will be available at a buyout price.
A partnership track offer should include, in writing:
- Timeline to partnership (e.g., “option to purchase 40% equity after 36 months”)
- Valuation methodology for the equity purchase
- Performance milestones required to trigger the option
- Whether the associate is building goodwill credit during the associateship
Verbal partnership promises are not enforceable. If a partnership track is a factor in your compensation decision, get the terms in writing as part of the original employment agreement.
For a complete overview of financial management guides and resources, visit our Dental Practice Finances resource library.
For related reading, see our guide on comparing associate compensation under DSO employment vs. private practice.
For related reading, see our guide on how hygienist compensation structures compare to associate dentist models — and why it matters for retention.
Frequently Asked Questions
What is a fair percentage for an associate dentist?
25–32% of production is the current market range for most general dentistry associate positions. Below 25% is below market and difficult to recruit for. Above 35% production percentage typically requires exceptional associate productivity or specialist-level skills to be sustainable for the practice owner.
How do DSO associate compensation packages compare to private practice?
DSOs typically offer higher base salaries ($160,000–$200,000+ for experienced providers), with structured benefits packages including 401(k) matching and complete health insurance. However, DSO production percentages tend to be lower (22–28%), and providers have less clinical autonomy and scheduling control. The trade-off is security and benefits vs. upside and autonomy.
What does the term “adjusted production” mean in associate contracts?
Adjusted production is production after subtracting certain costs — most commonly lab fees. A contract paying “30% of adjusted production” deducts lab fees before calculating the associate’s percentage. This is standard and reasonable; the practice owner is not retaining profit on lab work. Always ask whether lab fees, supply costs, or other deductions are subtracted before the percentage is applied.
How often should associate compensation be reviewed?
Annually at minimum, with a formal review of production data, patient satisfaction metrics, and market benchmarks. Providers growing their skills and increasing production should expect incremental percentage increases or bonus structure improvements every 1–2 years. Practices that don’t conduct regular reviews lose associates to competitors who offer better transparency.
For related reading, see our guide on dental practice economics.
Is it better to hire an associate as an employee or independent contractor?
In most dental practice situations, clinicians who work regular hours in your facility, using your equipment, under your supervision, meet the IRS and state definitions of an employee — not an independent contractor. Misclassifying an associate as a contractor exposes the practice to significant back-tax liability, penalties, and potential labor law violations. Consult an employment attorney before setting up any independent contractor arrangement with a regularly scheduled associate.