TL;DR — Key Takeaways
- A growing dental practice tracks five core metrics: new patient count, case acceptance rate, production per visit, patient retention, and overhead percentage.
- Independent practices earning $750K–$1.5M in annual collections have the best combination of growth runway and operational control.
- Case acceptance rate is the single highest-use variable — moving from 55% to 70% adds more revenue than doubling your new patient flow.
- Operational overhead above 65% signals a structural problem that no amount of new patients will fix.
- DSOs control roughly 25–30% of dental offices in the U.S. — independent practices must compete on relationship and experience, not price.
- A realistic growth timeline: 12 months to stabilize systems, 24 months to see compounding retention gains, 36–48 months to optimize profitability.
Most dental practices don’t fail because dentists are bad clinicians. They stagnate because the owner never received a business education to match their clinical training — and running a practice without that education means flying blind on the metrics that actually determine whether you’re growing, plateauing, or slowly contracting.
For related reading, see our guide on dental practice economics.
This guide is written for the practice owner who wants a clear, honest framework for growth: what it looks like in numbers, which levers move the needle most, and how to sequence improvements so one investment builds on the last. We’ve synthesized data from the ADA Health Policy Institute, Bureau of Labor Statistics compensation surveys, and financial benchmarks published by dental-specific CPA firms to give you figures you can actually act on.
For related reading, see our guide on improving dental practice profitability.
For related reading, see our guide on associate dentist compensation models.
For related reading, see our guide on dental staff hiring and compensation.
For related reading, see our guide on HIPAA compliance for dental practices.
By the end, you’ll have a complete picture of dental practice growth strategies — from the KPIs you should monitor weekly to the long-term structural decisions that determine whether you’re building an asset or just buying yourself a job.
What Defines a Growing Dental Practice: Metrics and Benchmarks
Growth without measurement is just motion. Before you can engineer growth, you need to agree on what it means. For dental practices, genuine growth shows up across five interconnected dimensions — and healthy practices track all five simultaneously, not just revenue.
The Five Core Growth Metrics
1. New Patient Flow
New patients are the top of your growth funnel, but they’re also the most expensive to acquire. Industry benchmarks from dental practice consultants consistently put healthy new patient acquisition at 25–40 new patients per month for a solo general practice. Below 20 per month, a practice is likely shrinking in active patient count even if the schedule looks full — because attrition from patients who move, age out, or disengage naturally runs 10–15% annually.
For related reading, see our guide on growing through patient retention.
The quality of new patients matters as much as volume. New patients who arrive via referral from existing patients have a 2–3x higher lifetime value than patients who find you through paid advertising, because referred patients enter with a pre-existing trust relationship and accept treatment recommendations at higher rates.
For related reading, see our guide on building patient trust and relationships.
2. Case Acceptance Rate
Case acceptance is the percentage of diagnosed treatment that patients agree to complete. It’s arguably the most underappreciated growth metric in dentistry. The industry average hovers around 55–60%, which means nearly half of diagnosed treatment walks out the door.
Practices that move this number from 55% to 70% — without adding a single new patient — effectively grow their productive output by 27%. No marketing campaign, no new operatory, and no extended hours produces that kind of use. For a practice producing $800,000 annually at 55% acceptance, closing the gap to 70% means an additional $203,000 in completed treatment annually.
3. Production Per Visit
Also called production per appointment, this metric tells you how efficiently each chair hour is monetized. A solo general dentist ought to target $350–$500 per appointment depending on fee schedule, geographic market, and payer mix. Below $250 per appointment signals either a high volume of hygiene-only visits without restorative follow-through, or a fee schedule that hasn’t been updated in several years.
For related reading, see our guide on efficient dental clinic management.
4. Patient Retention Rate
Retention measures what percentage of active patients return within 18 months for their next scheduled appointment. Practices with strong systems typically maintain 85–90% retention. Every percentage point below 85% represents a significant revenue leak — because replacing a lost patient costs four to five times more than retaining one.
For a deep-examine the systems that drive retention, see our guide on growing your dental practice through patient retention.
5. Overhead Percentage
Overhead is the percentage of gross collections consumed by expenses before the doctor’s compensation. According to ADA Health Policy Institute data, the average dental practice runs at 75–78% overhead when doctor compensation is treated as an expense.[1] Subtract that compensation line out (i.e., look at operating overhead only), and well-run practices must be in the 55–65% range.
Any operating overhead above 65% warrants a systematic audit. Usually the culprits are: (a) under-priced fee schedules, (b) over-staffed front desk relative to patient volume, (c) supply costs not negotiated in years, or (d) lab fees exceeding 10% of collections.
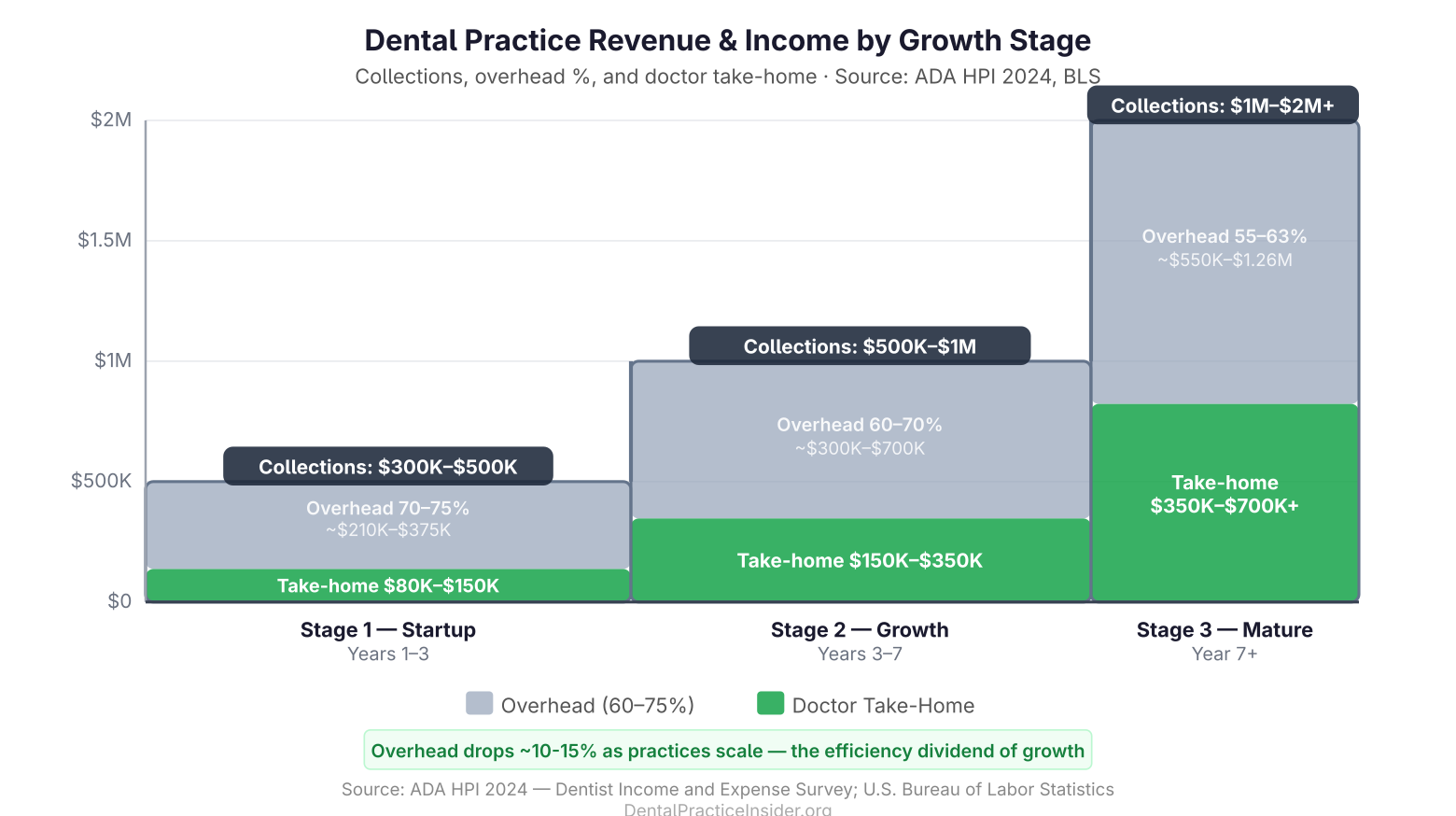
Revenue Benchmarks by Practice Stage
| Stage | Annual Collections | Operating Overhead Benchmark | Doctor Take-Home Range |
|---|---|---|---|
| Startup / Early (Years 1–3) | $300K–$500K | 70–75% | $80K–$150K |
| Growth Phase (Years 3–7) | $500K–$1M | 60–70% | $150K–$350K |
| Mature / Optimized (Year 7+) | $1M–$2M+ | 55–63% | $350K–$700K+ |
According to Bureau of Labor Statistics Occupational Employment data, the median self-employed dentist earns approximately $180,000–$230,000 annually, but the distribution is wide — high-performing practice owners routinely earn $400,000–$600,000+, while practices stuck in the startup phase can pay their owner less than a senior associate.[2]
Setting Strategic Goals for Your Practice
Growth doesn’t happen by trying harder. It happens by committing to specific, measurable targets and building your systems backward from those targets. Vague aspirations like “grow the practice” or “attract more patients” produce vague results. Operational goals produce operational change.
The SMART Framework, Applied to Dentistry
SMART goals — Specific, Measurable, Achievable, Relevant, Time-bound — are the standard because they work. But most dental practices apply the framework at the wrong level. Setting a goal to “increase revenue by 20%” is SMART on paper but useless in practice because revenue is the result of dozens of upstream variables. Instead, set SMART goals at the level of those upstream variables:
- Specific: “Increase case acceptance rate from 57% to 68% by Q4 2026”
- Measurable: Track acceptance weekly using practice management software reports
- Achievable: Based on current diagnosis rate and known treatment presentation gaps
- Relevant: Case acceptance is the primary constraint on production growth
- Time-bound: Committed to a specific quarter with monthly check-ins
Annual Goal Categories for a Dental Practice
A complete practice goal structure should include targets in at least four categories:
Production and Collections Goals
Set both gross production and net collections targets. Collections ought to be 97–99% of production after adjustments for a well-managed billing process — anything below 95% signals unresolved insurance claim delays, excessive write-offs, or poor front desk follow-through on accounts receivable.
Patient Base Goals
Define both volume targets (new patients per month) and composition targets (what percentage of new patients must be new to your market versus reactivated patients versus referrals). Tracking composition tells you which acquisition channels are actually working.
Operational Efficiency Goals
Metrics like same-day cancellation rate (target: below 6%), hygiene reappointment rate (target: 95%+), and average days in accounts receivable (target: below 30 days) are the operational substrate of a growing practice. For a systematic framework for managing these, see our overview of efficient management techniques for dental clinics.
Team Development Goals
What CE hours per team member, what cross-training certifications, and what staff retention rate are you targeting? High-performing practices budget 2–3% of gross production for team training and development — and they treat it as a revenue investment, not an overhead expense, because trained teams produce measurably better case acceptance and patient satisfaction scores.
The Morning Huddle as a Goal-Execution System
Goals don’t execute themselves. The single most effective implementation structure in a dental practice is the daily morning huddle: a 10–15 minute team meeting before the first patient that reviews the day’s schedule, flags opportunities (incomplete treatment in records, due-for-recall patients, unscheduled treatment plan line items), and assigns ownership of specific outcomes for the day. Practices that run consistent morning huddles report 10–15% higher daily production compared to practices without them, according to dental practice management consultants at Productive Dentist Academy and similar training organizations.
For related reading, see our guide on morning huddle templates for dental practices.
Revenue Growth Strategies: New Patients, Case Acceptance, and Treatment Mix
Revenue growth in a dental practice comes from three sources, in this order of use: (1) increasing production from your existing active patient base, (2) increasing new patient flow, and (3) expanding the range of services your practice offers. Most owners pursue these in reverse order — chasing new patients first — which is why marketing spend often delivers disappointing returns.
Based on ADA HPI survey data and industry benchmarks we track for this guide, practices that move case acceptance from 55% to 70% generate more additional revenue than adding 20 new patients per month — without any increase in marketing spend. That is the highest-return growth lever available to most independent practice owners.
For related reading, see our guide on DSOs vs independent dental practices.
Maximizing Production From Your Existing Patient Base
Treatment Presentation and Communication
The gap between what you diagnose and what patients accept is almost always a communication problem, not a clinical one. Patients who don’t accept treatment usually fall into three categories: they don’t understand why the treatment is necessary, they don’t understand the consequences of declining, or they don’t have confidence that the financial obstacle is solvable.
Addressing category one requires visual aids — intraoral camera images, X-ray walk-throughs, side-by-side comparisons. Patients who see their problem accept treatment at significantly higher rates than patients who are told about it. Studies cited by the ADA suggest intraoral camera use can increase case acceptance by 30–50% for the specific conditions visualized.[3]
Addressing category three requires presenting financing and payment options proactively, not reactively. Offering a third-party financing option (CareCredit, Sunbit, or in-house payment plans) before the patient raises cost as a concern removes a significant barrier. Practices that present financing as a standard part of the treatment presentation — not as a consolation after the patient hesitates — see meaningfully higher acceptance for multi-visit treatment plans.
Reactivating Dormant Patients
The cheapest new patient you can find is already in your practice management software. Patients who haven’t been seen in 12–24 months represent an enormous, low-cost opportunity. A systematic reactivation campaign — targeted outreach by phone and text to patients with overdue appointments or incomplete treatment — consistently generates $30–$80 in additional production per dollar spent on outreach, depending on the practice’s unscheduled treatment backlog.
For related reading, see our guide on essential dental practice technology.
New Patient Acquisition Strategies
Referral Systems
Internal referrals — patients sending friends and family — are the highest-converting, highest-retention source of new patients. Yet most practices operate with no formal referral system. A basic system includes: thanking every referring patient by name (a personal note costs nothing), tracking which patients refer and how frequently, and making the referral process easy (referral cards, a simple sentence your team says at checkout).
Specialty referrals — from oral surgeons, orthodontists, periodontists — can generate 5–20 new patient referrals per month for a general practice willing to build those relationships systematically. Monthly specialist lunches, coordinated treatment notes, and prompt communication on referred patients’ outcomes build the kind of professional trust that sustains two-way referral relationships.
Online Presence and Reputation
According to a survey by Software Advice, 71% of patients use online reviews as their first step in finding a new dentist. A practice with fewer than 50 Google reviews — regardless of rating — is functionally invisible to new patients conducting research. Generating reviews requires a system: a prompt at checkout, a text message with a direct link, and a staff member trained to respond to every review within 48 hours.
Local SEO is the other component. A fully optimized Google Business Profile with accurate hours, service categories, photos, and consistent name/address/phone across all directories will outperform a thousand-dollar monthly ad spend for high-intent searches like “dentist near me” or “dental office [city].”
Treatment Mix and Service Expansion
Adding services to an existing practice generates higher margins than new patient acquisition because you’re monetizing existing relationships. The highest-margin service additions for a general dentist are typically:
- Clear aligner therapy (Invisalign, ClearCorrect): Average case value $3,500–$6,000; production typically captured without adding operatory time
- Implant placement: Average case value $3,000–$5,000 per implant; requires surgical training but eliminates specialist referral revenue losses
- Sleep apnea appliances: Average appliance revenue $1,500–$3,000; increasingly covered by medical insurance; leverages existing patient relationships
- In-office whitening and cosmetic consultations: Lower revenue per case but high patient satisfaction and minimal chair time
The key discipline when adding services is not to chase revenue for its own sake. Add a service only if: (a) you have the training to deliver it at a quality level you’re proud of, (b) there’s demonstrated demand in your existing patient base, and (c) you can support the clinical workflow without degrading your core services.
Operational Efficiency Improvements That Directly Impact Profitability
Operational inefficiency is invisible overhead. Unlike a supply bill or a payroll run, the cost of a disorganized schedule, a broken cancellation policy, or a billing department that doesn’t follow up on claims doesn’t show up as a line item — it just quietly reduces your collections every single month.
Schedule Optimization
A dental schedule should be structured, not just filled. The difference is intentional sequencing: high-production procedures scheduled during peak provider energy (typically mid-morning), hygiene appointments distributed to maintain consistent floor traffic, and buffer time built in for same-day treatment opportunities. A practice running a fully reactive schedule — filling gaps as they appear without a sequencing philosophy — consistently underperforms its production potential by 15–25%.
Key scheduling KPIs to monitor:
- Same-day cancellation rate (target: below 6% of scheduled appointments)
- No-show rate (target: below 3%)
- Unscheduled time as percentage of available chair hours (target: below 10% for a mature practice)
- Hygiene reappointment rate at time of checkout (target: 95%+)
Accounts Receivable and Billing
The average dental practice has 60–90 days of production sitting uncollected in accounts receivable at any given time. For a practice producing $100,000 per month, that’s $180,000–$270,000 that has been earned but not yet collected — a significant working capital drag.
Insurance claims ought to be submitted same-day or within 24 hours of treatment. Claims not paid within 30 days require active follow-up. Patient balances must trigger automated statements at 30 days and personal phone contact at 60 days. Practices with these systems in place typically collect 98–99% of adjustable production; practices without them commonly see collection rates of 92–95%, representing a permanent revenue loss of 3–7% of gross production.
For a detailed breakdown of the financial systems that underpin profitable practice economics, see our guide on mastering the economics of dental practice management.
Supply Chain and Lab Cost Management
Dental supplies should run between 5–7% of gross collections. Lab fees ought to stay below 10%. Together, these two categories — supplies and lab — must represent 12–17% of collections for a well-managed practice. Practices above 17% in this combined category have almost always failed to: (a) negotiate vendor contracts in the last 2–3 years, (b) standardize material selections to reduce SKU count and increase negotiating use, or (c) audit lab relationships relative to the market.
Annual supply contract renegotiation — even if you’re satisfied with your current vendor — consistently yields 8–15% savings for practices willing to get competing quotes and use them as use.
Building a High-Performing Dental Team
The single greatest operational risk for a growing dental practice is staff turnover. The Bureau of Labor Statistics reports dental assistant turnover rates averaging 30–40% annually at the industry level — meaning a practice loses, on average, its entire dental assistant team every 2–3 years.[2] Each departure costs an estimated $15,000–$25,000 in recruiting, onboarding, and lost productivity, according to dental HR consultants.
Hiring for Culture and Attitude, Training for Skill
Clinical skills can be taught. Attitude, work ethic, and patient empathy are far harder to develop post-hire. The highest-performing dental teams are built by practices that define their culture explicitly — what behaviors they reward, what standards are non-negotiable, what values are lived day-to-day — and hire against that culture.
A structured interview process with behavioral questions (“Tell me about a time a patient was upset — how did you handle it?”) predicts on-the-job performance far better than credentials and experience alone. Reference checks, working interviews where candidates interact with actual patients, and a 90-day onboarding program with clear performance milestones reduce bad hires dramatically.
Compensation and Retention Strategy
Paying at or above market is a prerequisite for attracting strong team members, but it’s not sufficient for retaining them. The research on dental team retention consistently identifies three drivers that matter more than salary once baseline compensation needs are met:
- Leadership quality: Team members leave managers, not companies. A dentist owner who communicates clearly, handles conflict professionally, and recognizes contributions consistently retains staff regardless of whether they’re the highest-paying office in the market.
- Growth opportunity: Cross-training, CE support, and a visible career path signal that the practice is investing in the individual. Front desk staff promoted to treatment coordinator roles, for example, become deeply loyal because they know that advancement is possible.
- Team cohesion: Practices that invest in team-building — retreats, shared goals, transparency about practice metrics — create a sense of collective ownership that pays dividends in discretionary effort.
Performance Management
Team members perform best when they know what’s expected, receive regular feedback, and understand how their individual contribution connects to practice goals. Annual performance reviews are insufficient — they should be supplemented with monthly individual check-ins (even 15-minute conversations), weekly team huddles that share production data, and quarterly goal reviews where team members assess their own progress against agreed targets.
Technology and Systems That Support Sustainable Growth
Technology is not a growth strategy. Technology is an enabler of strategies that are already working. Practices that invest in technology without first fixing their processes and systems typically find that the technology amplifies their existing dysfunction rather than solving it.
With that caveat in mind, there is a core technology stack that every growing dental practice ought to have in place:
Practice Management Software
Your practice management software (Dentrix, Eaglesoft, Curve, Open Dental, Carestream) is the operational nerve center of your practice. Every metric discussed in this guide — case acceptance rate, production per visit, recall compliance, AR aging — must be available as a scheduled report from your PMS. If you’re not running weekly production reports, you’re managing your practice on intuition rather than data.
Practice management software has a search volume of nearly 10,000 monthly searches from dental professionals, which indicates the high interest in this category — and the wide variation in platforms in use across the industry. If you’re evaluating or switching platforms, prioritize: report depth, billing integration, and support quality over feature count.
Digital Radiography and Intraoral Cameras
Both technologies should be considered foundational, not premium — they pay for themselves through case acceptance improvements alone. Intraoral cameras in particular are one of the highest-ROI investments a practice can make: they turn an invisible diagnosis into a visible problem the patient can see and understand, directly driving treatment acceptance.
Patient Communication Platforms
Automated patient communication — appointment reminders by text, recall outreach, post-treatment follow-up, review request sequences — is one of the most leveraged investments in a growing practice because it scales without adding staff time. Platforms like Weave, Birdeye, RevenueWell, and NexHealth handle most of these functions and typically pay for themselves through no-show reduction alone.
Digital Workflow for Same-Day Dentistry
CAD/CAM systems (CEREC, Planmeca, Glidewell IO) enable same-day crown delivery, which eliminates temporaries, reduces broken appointments between preparation and delivery, and dramatically improves the patient experience for restorative work. The economics require careful evaluation — equipment costs are substantial — but practices with sufficient restorative volume (15+ crowns per month) typically see a strong return within 3–5 years through lab fee savings and production efficiency gains.
For a broader view of how post-pandemic operational shifts have changed technology expectations, see our analysis of adapting dental practices for the post-pandemic era.
For related reading, see our guide on modern dental practice management.
Financial Planning for Sustainable Practice Growth
A dental practice that grows revenue without managing the financial structure of that growth can end up in a worse position than if it had stayed smaller. Debt service on equipment loans, increased payroll ahead of confirmed production, and expansion costs that outpace collections growth are all traps that have claimed well-intentioned practices.
Building a Practice Budget and Financial Model
Every practice ought to operate from an annual budget that projects monthly revenue, fixed expenses, variable expenses, and owner compensation. The budget is not a forecast — it’s a commitment, a deliberate allocation of expected resources that creates accountability. Actual versus budget variance reviews (monthly, at minimum) tell you where your assumptions were wrong and let you make corrections before small variances compound into large problems.
Key financial ratios to monitor:
- Collections as % of production: Aim 97–99%
- Staff expenses as % of collections: Target 22–28% (includes wages, benefits, taxes)
- Occupancy as % of collections: Goal 5–10%
- Supply + lab as % of collections: Benchmark 12–17%
- Marketing as % of collections: Target 2–5% for a growing practice
- Doctor compensation as % of collections: Objective 35–45% for a solo owner
Fee Schedule Management
One of the most consistently overlooked levers in dental practice economics is the fee schedule. Many practices have not meaningfully updated their fees in 3–5 years, which means their effective revenue per procedure has declined in real terms after inflation. A fee schedule audit — benchmarking your current fees against the 75th percentile of usual, customary, and reasonable fees for your geographic market — must be an annual event, not a reactive response to financial pressure.
Implementing a fee increase requires a clear communication plan for patients on out-of-pocket care and careful analysis of any insurance contract provisions that cap your ability to increase fees. For practices with high PPO participation, fee schedule increases may require renegotiating contracts or making strategic decisions about which insurance relationships to maintain.
Practice Loans and Debt Management
Debt is a growth tool when used correctly and a growth inhibitor when not. Equipment loans, practice acquisition financing, and expansion loans all carry different risk profiles and should be evaluated against realistic production projections, not optimistic ones.
A general rule: total practice debt service (all loan payments per month) ought to not exceed 8–10% of monthly gross collections. Practices carrying debt service above this level have limited flexibility to weather revenue shortfalls and are constrained in their ability to invest in additional growth drivers.
For a detailed look at how financial strategy connects to practice profitability, read our pillar on improving dental practice profitability.
Building Practice Value as a Business Asset
Practice value is typically calculated as a multiple of EBITDA (earnings before interest, taxes, depreciation, and amortization) or as a percentage of annual gross collections. The industry standard for general practice valuations runs between 60–85% of trailing 12-month gross collections, with the multiple adjusting based on growth trajectory, location, payer mix, staff stability, and physical plant condition.
A practice owner who understands valuation methodology makes different decisions than one who doesn’t. Investing in systems that improve recurring patient retention, reducing insurance dependency, and building a team that can function without the owner’s daily presence all add measurable value to the business — because they make it more attractive to a future buyer or successor dentist.
Managing DSO Competition as an Independent Practice
Dental Service Organizations now control an estimated 25–30% of dental offices in the United States, with ownership concentration continuing to grow at a rate of 3–5 percentage points per year according to industry analysis from the American Dental Association [1] Health Policy Institute.[1] In major metropolitan markets, DSO-affiliated practices may represent 40–50% of all offices.
For an independent practice owner, this is a material competitive reality — not a distant threat. DSOs compete on convenience (extended hours, multiple locations), price perception (network insurance participation), and marketing budget (centralized digital advertising at scale that individual practices cannot match). An independent practice that tries to compete on these same dimensions will lose. The winning strategy is differentiation.
Where Independent Practices Win
Continuity of Care
DSO-affiliated practices often have higher associate turnover and inconsistent patient-to-provider relationships. An independent practice where the owner is present, knows patients by name, and maintains relationships across years has a fundamentally different value proposition — one that a significant segment of patients will pay a premium for and actively refer others to.
Clinical Decision-Making Autonomy
Independent practice owners make clinical decisions without a management layer reviewing production metrics and suggesting treatment protocols. For patients who have experienced over-treatment or have concerns about corporate dental chains, an independent practice’s ownership transparency is a genuine differentiator — one worth communicating explicitly in your marketing.
Community Embeddedness
A practice that has been part of a community for 10–20 years, participates in local events, sponsors school programs, and treats multiple generations of the same families has a competitive moat that no marketing budget can replicate. DSOs are businesses; community practices can be institutions. That distinction is valuable and must be cultivated intentionally.
Strategic Options for Independent Practices
Some practice owners facing DSO competition choose to join rather than compete. This is a legitimate strategic decision that deserves rigorous analysis rather than reflexive rejection. DSOs vary enormously in their management culture, clinical autonomy provisions, and financial structures. Some affiliations allow dentists to retain meaningful autonomy while gaining administrative relief; others represent a fundamental loss of control.
For a thorough analysis of how DSOs are reshaping the industry and what it means for independent owners, see our complete guide on understanding the impact of DSOs on the dental industry. For practices considering the transition away from PPO-dependent revenue as part of a differentiation strategy, see our guide on reducing insurance dependency in dental practices.
Growth Timeline and Realistic Milestones
Growth takes longer than expected and compounds faster than expected — but only if the foundational systems are in place. Here is a realistic milestone framework for a general dental practice pursuing deliberate, systematic growth:
Year 1: Foundations and Systems
The primary work in the first year of a growth initiative is diagnostic and structural. You need to know your actual numbers before you can improve them, and you need functional systems before you can scale. Key milestones:
- Complete a full financial audit: identify your current overhead percentage, accounts receivable aging, and collection rate
- Benchmark your five core metrics against industry standards (see the opening section of this guide)
- Implement or optimize a morning huddle system with weekly team metrics review
- Conduct a fee schedule benchmark analysis; implement a fee increase if warranted
- Identify and address the single largest operational bottleneck (usually scheduling or billing)
- Build or audit your Google Business Profile and online review presence
Year 2: Compounding Gains
With systems in place, year two is when the compounding effect of patient retention starts to show up in your numbers. Patients who were retained in year one refer new patients. Hygiene recall compliance improves as your reminder systems mature. Case acceptance gains from improved treatment presentation translate into restorative production. Key milestones:
- Goal 3–5 percentage point improvement in case acceptance rate from year-one baseline
- Achieve recall compliance rate of 85%+ for active patients
- Reduce same-day cancellation rate to below 6% through improved confirmation protocols
- Launch or optimize a formal patient referral recognition system
- Complete cross-training initiatives so no single critical function has a single point of failure
Year 3 and Beyond: Optimization and Expansion
A practice that has strong systems, good retention, and a managed overhead structure in years one and two is in a position to grow aggressively in year three without the risk of the growth itself creating operational chaos. Expansion of services, second-chair utilization, additional providers, or multi-location considerations all become viable when the foundation is solid. Key milestones:
- Evaluate and potentially implement one new high-value service (clear aligners, implants, sleep appliances)
- Assess associate dentist hiring if producer utilization exceeds 85% of available chair time
- Conduct a formal practice valuation to understand current enterprise value and benchmark future decisions
- Develop a 5-year strategic plan that includes a personal financial planning component for the owner
Frequently Asked Questions: Dental Practice Growth
- What is a good growth rate for a dental practice?
- A healthy annual revenue growth rate for an established general practice is 8–15% per year. Practices growing faster than 15% annually often have corresponding operational stress unless they have invested ahead of the growth in team, systems, and physical capacity. Practices growing below 5% annually are likely declining in real terms after inflation.
- How many new patients per month does a dental practice need?
- A solo general practice needs a minimum of 20–25 new patients per month to offset natural attrition and maintain a stable active patient base. Practices targeting active growth should aim for 35–50 new patients per month. The exact number depends on your current active patient count, retention rate, and practice capacity.
- What is the average dental practice revenue?
- According to ADA Health Policy Institute data, the median gross billings for a solo general dental practice in the U.S. run approximately $750,000–$900,000 annually, though wide variation exists by geographic market, practice age, and payer mix. Practices in high-cost urban markets and practices with strong fee-for-service or elective service mixes frequently exceed $1.5M.
- What does dental office strategic planning look like in practice?
- Effective dental office strategic planning involves an annual off-site review of the previous year’s performance data, a deliberate goal-setting session that covers production, patient base, operations, and team development, and then a cadence of monthly metric reviews against those goals. The plan ought to be documented and shared with the full team — growth is a team activity, not a solo one.
- What are the dental practice KPI benchmarks I must track?
- The primary KPIs for a dental practice are: new patients per month (target: 25–40), case acceptance rate (target: 65–75%), production per visit (target: $350–$500), patient retention rate (target: 85–90%), collection rate (target: 97–99%), and operating overhead (target: 55–65%). These six metrics, tracked weekly and monthly, give you an accurate and complete picture of practice health.
- How long does it take to grow a dental practice?
- With systematic effort, most practices see meaningful metric improvement within 12 months, tangible production gains within 18–24 months, and significant financial outcomes — improved profitability, reduced owner hours, or expanded capacity — within 36–48 months. Practices that pursue growth opportunistically rather than systematically often spend years doing the same things and getting the same results.
- Should I join a DSO or stay independent?
- This depends entirely on your personal goals, financial situation, and what you want your professional life to look like. DSO affiliation can provide genuine administrative relief, capital access, and marketing scale. Independence provides clinical autonomy, practice ownership equity, and the ability to build a long-term patient relationship model. Neither is inherently superior — the right answer is the one aligned with your goals. Both paths can produce excellent financial outcomes for dentists who pursue them intentionally.
The Path Forward: Building a Practice That Grows Intentionally
Dental practice growth is not a mystery. The practices that grow consistently are not the ones with the most aggressive marketing budgets or the most advanced technology suites — they’re the ones that understand their numbers, manage their systems, develop their teams, and make decisions based on data rather than instinct.
The framework in this guide gives you the measurement tools, the strategic priorities, and the timeline expectations to approach growth as a professional discipline. The next step is choosing one thing — not ten things, one thing — and executing on it with the same precision you bring to a complex clinical case.
Start with your case acceptance rate. Pull the report from your practice management software. Find out what your number actually is. Then read our guide on patient retention — because retention and case acceptance are more closely connected than most owners realize — and build from there.
Growth compounds. The practices you admire didn’t get there in a single year. They got there by making better decisions, one quarter at a time, for a long time. You can do the same.
Sources and References
- American Dental Association Health Policy Institute. Dentist Income and Dental Practice Revenue: A Survey of U.S. Dentists. ADA.org/hpi. Accessed March 2026.
- U.S. Bureau of Labor Statistics. Occupational Employment and Wage Statistics: Dentists, All Other Specialties. BLS.gov/oes. Accessed March 2026.
- American Dental Association. Intraoral Camera Use and Case Acceptance: Clinical Practice Observations. ADA.org. Accessed March 2026.