Dental hygiene is the revenue engine and patient relationship foundation of most general dental practices — and it is consistently the most under-managed department. The department typically represents 25–35% of total practice collections, and the clinical team maintains the recall relationships that produce the treatment diagnoses feeding the restorative schedule. When this department underperforms — through staffing instability, recall leakage, or operational friction — the entire practice feels it. This guide addresses the most common dental hygiene challenges practice owners face and the operational solutions that resolve them.
For related reading, see our guide on dental practice growth strategies.
For related reading, see our guide on building patient trust and relationships.
What Are the Biggest Dental Hygiene Challenges for Practice Owners?
Based on ADA Health Policy Institute surveys and practice management research, these are the challenges practice owners rank as most operationally disruptive:
For related reading, see our guide on dental practice marketing strategies.
For related reading, see our guide on visual aids for patient education.
- Hygienist recruitment and retention in a tight labor market
- Reappointment leakage — patients not rescheduling between preventive care appointments
- Under-diagnosis in the operatory — pathology identified but not presented
- Production benchmarks not being met despite full schedules
- Inconsistent clinical protocols across team members
- Periodontal coding and documentation gaps
- Patient compliance with treatment recommendations
Each of these challenges has operational solutions. They are not permanent features of running a hygiene department — they are management problems.
How Do You Recruit and Retain Dental Hygienists?
The staffing shortage is structural. The Bureau of Labor Statistics projects dental hygienist employment to grow 9% through 2032 — faster than average — while the number of new graduates from accredited programs has grown more slowly than demand. In many markets, qualified hygienists receive multiple recruitment inquiries per month.
Retention is the most cost-effective response. Replacing a hygienist costs an estimated $10,000–$20,000 in recruitment, onboarding, and productivity loss during the learning curve — before accounting for the patient attrition that often accompanies staff turnover in this department, since patients frequently have strong personal relationships with their hygienist.
Retention strategies that matter most to your preventive care team:
- Realistic time per patient. Scheduling 40-minute appointments when 60 minutes of thorough care is needed creates chronic resentment and shortcuts. If your hygienists are consistently running behind because of inadequate appointment length, this is your most urgent retention problem.
- Equipment that works. Ultrasonic scalers, digital x-ray, and functional air/water syringes are not luxuries — they are the tools hygienists need to do their job competently. Outdated or unreliable equipment signals that the owner doesn’t respect the clinical role.
- Autonomy over clinical protocols. Team members who are trusted to make appropriate clinical decisions — recommending additional radiographs when warranted, adjusting appointment frequency based on patient risk, recommending adjunct therapies — report higher job satisfaction than those who feel micromanaged.
- Competitive compensation with clear advancement. Compensation should be reviewed annually against your local market rate. The ADA and ADHA both publish salary surveys that provide benchmarking data. A hygienist who is underpaid relative to the market and has no visible path to advancement will eventually leave.
How Do You Solve the Reappointment Leakage Problem?
Reappointment leakage — patients completing a hygiene appointment without scheduling their next one — is the most financially costly and least recognized hygiene department problem in most practices. Consider the math: if your preventive department sees 400 patients per month and 20% fail to reschedule (a conservative estimate for practices without a structured recall system), you’re losing 80 appointments per month. At $150–$200 per visit, that’s $12,000–$16,000 in monthly revenue that should be yours.
Structural fixes:
- Pre-appoint at checkout. The highest-performing practices have a 95%+ same-day reappointment rate. The hygienist or checkout coordinator books the next appointment before the patient leaves the chair. “Let’s get you scheduled for your next visit — do you prefer mornings or afternoons?” is a script, not a question.
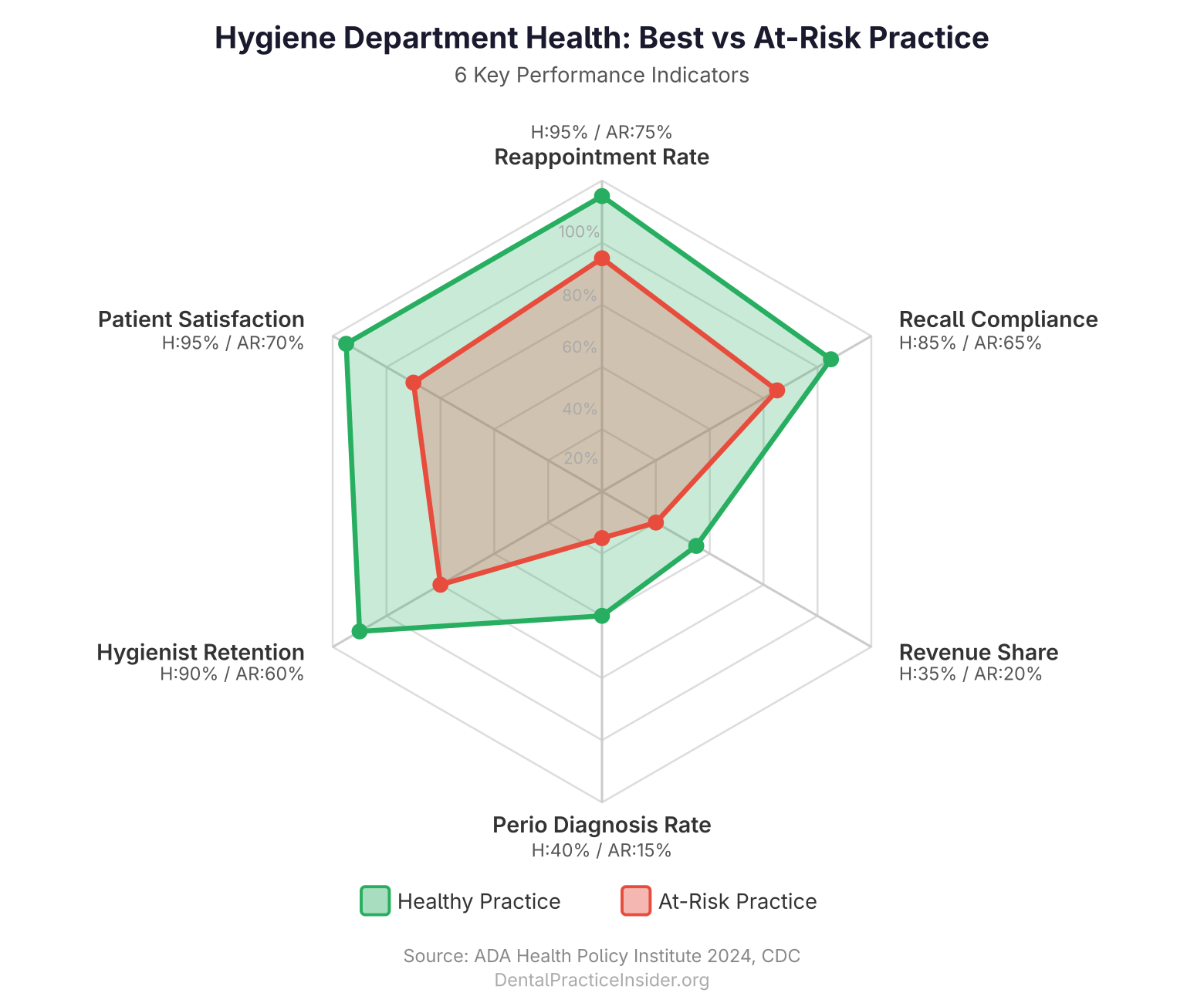
- Track reappointment rate monthly. If you don’t measure it, you can’t manage it. Benchmark: 85% or higher. Below 80% is a systemic problem.
- Active recall outreach. For patients who leave without scheduling, a three-contact outreach sequence — phone call, text, email — within the first 2–4 weeks post-appointment recovers a significant percentage. Automated systems (Lighthouse 360, Dentrix Ascend recall, Recare systems) handle this at scale without staff time.
- Recall interval communication. Patients who don’t understand why they need to return in 3 months (rather than 6) don’t prioritize the appointment. Clear explanation of patient-specific risk factors — “Your bone levels and pocket depths indicate we should monitor you more closely than a patient with no history of gum disease” — creates compliance through understanding.
How Do You Improve Preventive Care Production?
Low department production despite full schedules almost always traces to one of three root causes: under-coding, undertreated periodontal disease, or missed adjunct therapy opportunities.
Periodontal Protocol Consistency
Inconsistent probing and staging is the most common production gap in hygiene. Practices that consistently probe, stage and grade periodontitis (per the 2017 AAP/EFP classification), and document appropriately have dramatically higher periodontal coding rates than those that don’t. The treatment itself — scaling and root planing, localized antimicrobial therapy, supportive periodontal therapy recalls — generates significant additional production per patient.
A simple audit: pull your hygiene production for the past 90 days and calculate what percentage of patients received prophylaxis codes versus periodontal codes. If the percentage of periodontal codes is significantly below the estimated disease prevalence in your market (the CDC estimates 47% of adults 30+ have some form of periodontal disease), your team may be under-diagnosing or under-documenting.
Adjunct Therapy Utilization
Fluoride varnish, antimicrobial irrigation, and sealants are all clinically appropriate for segments of the patient population and represent legitimate additional production. Practices with clear protocols for which patients should receive which adjunct therapies — and hygienists who are empowered to offer them — produce significantly more per clinical hour than those without protocols.
How Do You Ensure Consistent Clinical Protocols Across Your Preventive Team?
As practices grow and add team members, protocol inconsistency becomes a patient safety and production issue. Patients who see different providers over time should receive the same standard of care — same probing documentation, same radiograph protocol, same risk assessment conversation — regardless of which team member treats them.
Creating consistency:
- Document clinical protocols in writing for each category of hygiene appointment type
- Conduct quarterly case review meetings where hygienists present cases and discuss management approaches
- Standardize risk assessment tools (CAMBRA for caries, AAP staging for periodontal) so all hygienists are using the same framework
- Audit production and coding by clinician quarterly — significant variation between providers is a diagnostic signal worth investigating
How Does Preventive Care Connect to the Restorative Schedule?
The department’s most important function may be diagnostic rather than therapeutic. Hygienists who are probing thoroughly, monitoring existing restorations, and presenting findings to the doctor produce a steady stream of diagnosed, un-started treatment — the inventory that fills the restorative schedule weeks and months ahead. Hygienists who rush through appointments without this diagnostic rigor leave this pipeline empty.
Building this connection explicitly:
- Morning huddles should include review of preventive appointments with anticipated diagnoses
- Doctor exam timing during these appointments should allow enough time for a genuine conversation about findings
- Hygienists should be oriented to understand that their diagnostic work translates directly into patient health and practice production — they are not just cleaning teeth, they are producing the clinical intelligence that drives the restorative schedule
A well-functioning hygiene department is the most reliable driver of dental practice profitability. It is also, when properly supported, one of the most rewarding parts of a practice to lead — because the patient relationships hygienists build over years of consistent care are at the heart of what makes an independent practice irreplaceable to its community.
For related reading, see our guide on the staffing side of sustaining a high-performing hygiene department.
Key Takeaways
- Hygiene represents 25–35% of total practice collections; it is the most under-managed revenue driver in most practices.
- Replacing a hygienist costs $10,000–$20,000; the primary retention levers are realistic appointment time, functional equipment, clinical autonomy, and market-rate compensation.
- A 20% recall leakage rate costs practices $12,000–$16,000 per month in hygiene production; same-day pre-appointment and automated recall outreach are the fixes.
- Inconsistent periodontal probing and staging is the most common hygiene production gap — audit your periodontal coding rate against CDC prevalence data.
- Morning huddles linking hygiene diagnoses to the restorative schedule are the operational connection most practices are missing.
For more resources on this topic, see our complete guide to dental practice management.